
Alex Rabindranath
April, 2013
3-Point Hip Abduction With a Thera-band
Mobility and strength at the hip joint is essential for almost all sports, and in any activity that involves running, jumping, and quick accelerations. The specific motion of hip abduction; extending the upper and lower leg out laterally from the midline of the body, is especially important in sports. Hockey, which uses hip abduction and extension to push into and off from the ice, and soccer, which requires significant hip strength and coordination to kick, change directions, and control the ball successfully, are great examples of this (Thorborg et al., 2011).
In addition to the requirements of hip abductor strength for sport specific movements, they are also crucial in injury prevention. Individuals with chronic ankle instability (CAI) have been shown to have weaker gluteus maximus and gluteus medius musculature in the effected limb (Webster & Gribble, 2013). This imbalance in gluteal strength is hypothesized to lead to improper foot and ankle positioning, predisposing the individual to greater risk of future or repeated ankle injury (Webster & Gribble, 2013). Strengthening the hip abductors and external rotator muscles has been shown to alter the lower leg joint loading, which can reduce the risk of injury and shows the value of hip strengthening exercises in both rehabilitation and prevention of lower extremity injuries (Snyder et al., 2009).
Bilateral discrepancies in hip strength in soccer players have often been noted to be a hypothesized causal factor in groin injuries (Thorborg et al., 2011). Dominant-leg hip adductor strength has been shown to be higher than non-dominant leg adductor strength in soccer players, which can lead to imbalances that predispose them to injury (Thorborg et al., 2011). If one thinks to the primary motions involved in ball control and ball striking, it is clearly evident that hip musculature plays a crucial role in game play and success. Exercises like the 3-point hip abduction with a thera-band can be a great addition to training and rehab regiments as it focuses on improving hip abduction strength in multiple ranges of motion and can also increases stability in hip, knee and ankle of the planted leg.
Evidence linking reduced hip abduction and external rotation to sacroiliac joint pain is another concern which makes exercises that increase hip mobility and strength a must have in any rehabilitation program (Bussey, Bell & Milosavljevic, 2009). Exercises like the 3-point hip abduction may also have great potential for use in Eastern cultures, where kneeling and cross-legged sitting are required in everyday activities (Kapoor et al., 2008). Also, knee and hip arthroplasty patients are of great concern when considering daily activities and adequate hip and knee movement capabilities, and exercises that strengthen these muscles and joints are crucial for successful rehabilitation (Kapoor et al., 2009).
Whether looking for improvements in performance, aiding in rehab, or trying to prevent common injuries, hip strengthening exercises like the 3-point hip abduction are a great supplement to any program. Combing this exercise with other great hip and gluteal exercises like hip thrusts and glute bridges can be a great way to get an edge on your competition. In addition this exercises can be tailored specifically to specific sports; for example focusing primarily on the ‘out and back’ abduction position seen in Figure 1.2 and Figure 2, is a great way to improve hockey stride strength. The exercises can even be combined with sport specific drills, such as controlling a soccer ball in the same planes of motion as seen in the exercise (Figures 1.2 - 1.4).

Proper Form
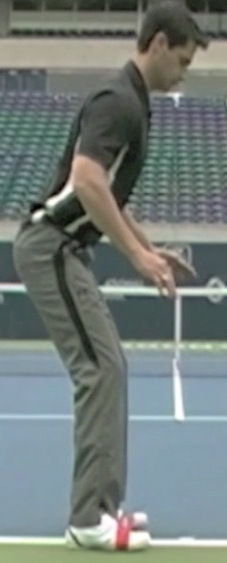
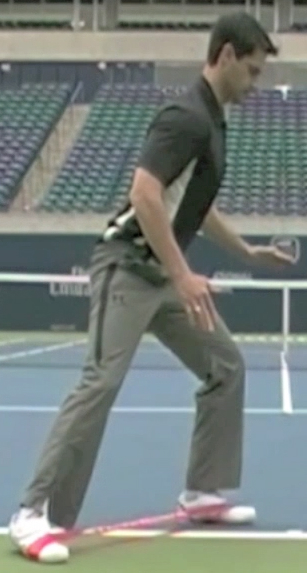
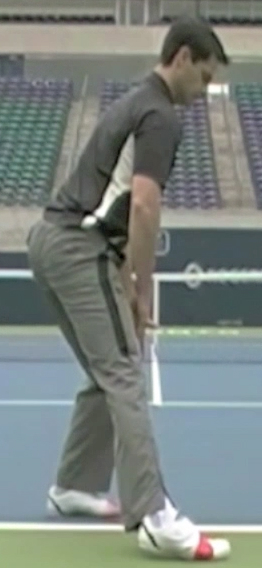
The 3-point hip abduction exercise is done with a thera-band wrapped around both feet in line with your baby toes. Starting in a ready position (Figure 1.1) the next steps are to abduct one leg to 3 different points; out and back (Figure 1.2), out to the side (Figure 1.3), and out and forward (Figure 1.4). In the ready position you want to have your butt sticking out slightly in an anterior pelvic tilt, and have a slight bend in the knees. Try to keep you waist as flat as possible when abducting to the 3 different positions. Bring your leg out as far as possible to these positions and make sure the abduction is coming from the hip.
You also want to make sure that the planted leg stays balanced and stable while the active leg is abducting. Keep the slight bend in the knee in the planted leg and try to maintain its position over your baby toe. This will help to increase stability and balance in the non-active leg while making sure that your glutes are activated. Keeping your waist as flat as possible throughout the exercise will also promote this.

Figure 2 - Hockey Stride (Adapted from www.hockeytutorial.com)
References
Bussey, M.D., Bell, M.L. & Milosavljevic, S. (2009). The influence of hip abduction and external rotation on sacroiliac motion. Manual Therapy, 14, 520-525.
Kapoor, A., Mishra, S.K., Dewangan, S.K. & Mody, B.S. (2008). Range of movements of lower limb joints in cross-legged sitting posture. The Journal of Arthroplasty, 23(3), 451-453.
Snyder, K.R., Earl, J.E., O’Connor, K.M. & Ebersole, K.T. (2009) Resistance training is accompanied by increases in hip strength and changes in lower extremity biomechanics during running. Clinical Biomechanics, 24, 26-34.
Thorborg, K., Couppe, C., Petersen, J., Magnuson, S.P. & Holmich, P. (2011). Eccentric hip adduction and abduction strength in elite soccer layers and matched controls: A cross-sectional study. British Journal of Sport Medicine, 45, 10-13.
Thorborg, K., Semer, A., Petersen, J., Madsen, T.M., Magnusson, P. & Holmich, P. (2011). Hip Adduction and Abduction strength profiles in elite soccer players. The American Journal of Sports Medicine, 39(1), 121-126.
Webster, K.A. & Gribble, P.A. (2013). A comparison of electromyopraphy of gluteus medius and maximus with and without chronic ankle instability during two functional exercises. Physical Therapy in Sport, 14, 17-22.