HIIT - A Smarter Way to Train
Alex Rabindranath
October, 2013
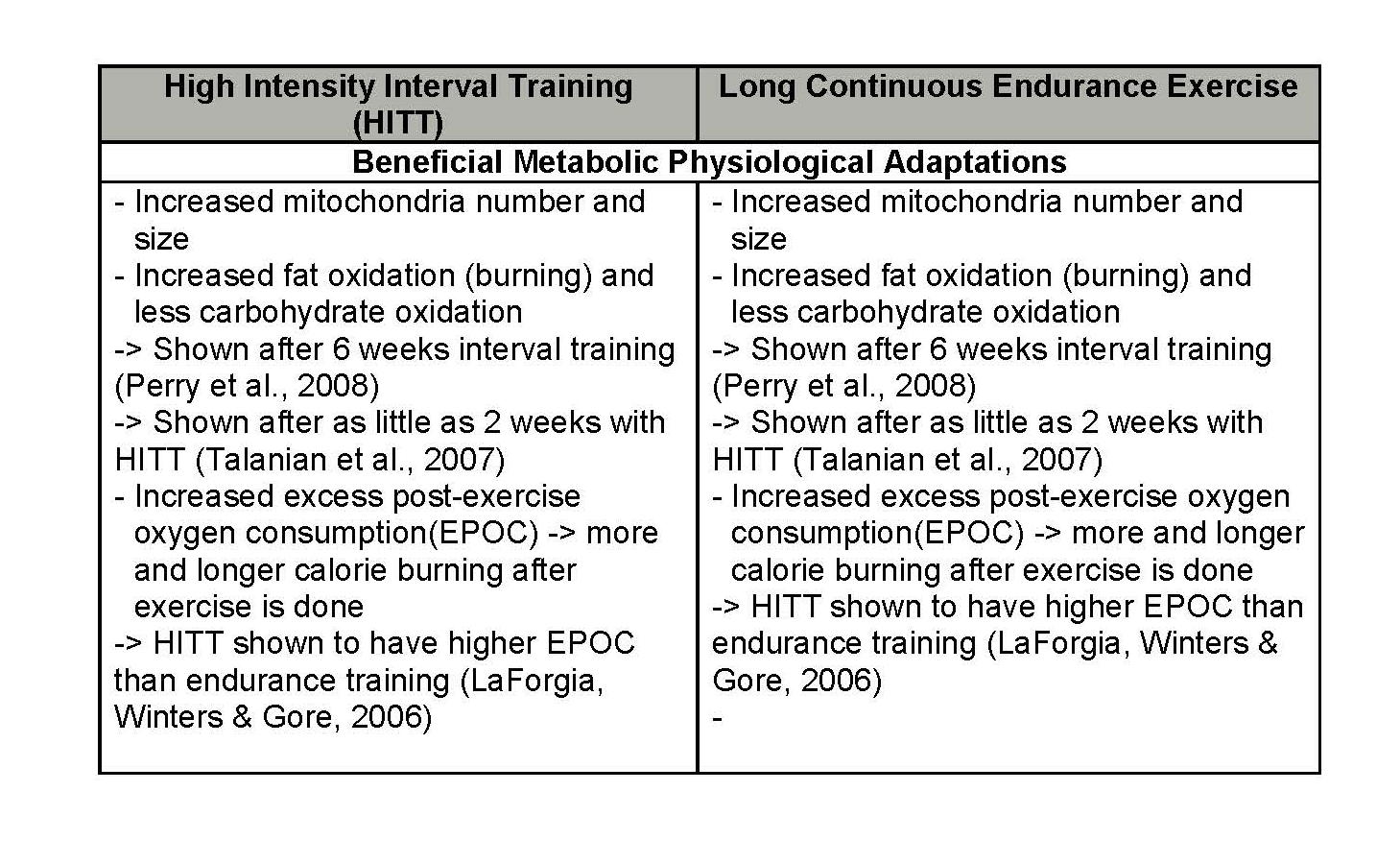
High Intensity Interval Training (HIIT) has been a hot topic of interest in fitness and physical activity in the last decade, being used and examined by professional athletes, recreational exercisers, and in clinical research. HIIT workouts consist of high intensity workloads (> 85% VO2Max – the maximal rate at which one’s aerobic systems can uptake and utilize oxygen effectively during exercise), done for a short duration (30 sec – 4mins), interspersed with recovery times in-between sets (Work:Rest ratios usually 1:1, 1:2 or 2:1). HIIT has been consistently shown to have similar, if not better, physical health benefits and improvements in performance when compared to traditional continuous endurance exercise (long runs, jogs, bike rides etc.) with a lower total volume of work done. In other words, HIIT programs allow for a shorter total workout time and volume, while producing similar or superior results to moderate intensity, long duration exercises (See charts below for HIIT benefits and a comparison to continuous endurance exercise – Zuhl & Kravitz, 2012).
Lack of time is a major barrier for most of the population when it comes to exercising and being physically active, as we all have many other responsibilities and commitments in our lives (school, work, family, friends, relaxing etc.). HIIT workouts can be a great asset when time constraints are present as athletic performance and many health benefits can all be achieved in a short period of time. Especially if your goals incorporate increasing your cardiorespiratory capacity (VO2Max), improving your body composition, or improving athletic performance, HIIT is definitely the way you’ll get the most ‘bang for your buck’.

In addition to these time saving and health related benefits, HIIT has also been shown to induce post-exercise oxygen consumption (EPOC), and to a greater degree than continuous endurance exercise (LaForgia, Winters, & Gore, 2006). Since HIIT consists of high intensity exercise, you will be using your anaerobic systems to provide energy during sets, which brings the body into a state of ‘oxygen debt’. Throughout the day after your workout, you will be burning more calories as your metabolism is increased to pay back this debt and to oxidize other by-products of using the anaerobic systems for energy, like lactic acid. So on top of the calories you will burn during your HIIT workout, you will also continue to burn calories afterwards for as long as 24-48 hours.

Many studies have shown that there is a marked increase in VO2Max, skeletal muscle oxidative capacity, and other athletic performance markers (higher vertical jump, faster 10m sprints etc.) from engaging in HIIT programs that last as little as 2-3 weeks (Acton-Jacobs et al., 2013; Bogdanis et al., 2013; Buchan et al., 2013; Tjonna et al., 2013). A recent study by Tjonna et al. (2013) found that an experimental group who participated in only one set of HIIT (one 4 minute set at 90% VO2Max, three sets/week for 10 weeks) showed similar improvements in weight loss and increased VO2Max to those who participated in more sets of the same HIIT protocol. This suggests that even engaging in minimal amounts of HIIT can be effective in improving cardiorespiratory fitness and overall health. Additionally, single sessions of HIIT have also been shown to increase transcription and biogenesis of mitochondria in skeletal muscle cells, even in highly trained athletes (Acton-Jacobs et al., 2013).
The majority of studies also show that HIIT is an excellent way to increase mitochondrial density and biogenesis in muscles, which also results in increased oxidative capacity (Acton-Jacobs et al., 2013; Boyd et al., 2013). Mitochondria are the ‘power-houses’ of cells and if their numbers are increased, more ATP (energy) can be synthesized and utilized by muscles. Simplified, this means that by increasing your mitochondrial content and oxidative capacity in skeletal muscles, you will be able to utilize oxygen more effectively and be able to work for longer at higher intensities, before having to rely on the anaerobic systems to provide energy. This is also known as increasing your anaerobic or lactic threshold.
As it is agreed upon that HIIT is one of the most effective ways to increase VO2Max, skeletal muscle oxidative capacity, and athletic performance, it is also agreed that performing workloads at higher/highest possible intensities results in the most robust improvements. The best benefits are usually obtained when working at 90% VO2Max or higher. Some sources propose that supramaximal intensities (>100%VO2Max) may be even more effective at improving aerobic and sprinting performance (Cicioni-Kolsky et al., 2013). In a review on HIIT, Buchhat & Laursen (2013) suggest that maximal/close to maximal intensities, as used in HIIT, are most effective at increasing aerobic capacity (VO2Max) because they stress the oxygen transport system the most, activate more and larger motor units of muscle fibers, and are performed at near maximal cardiac output. Moholdt et al. (2013) also report that regardless of frequency, duration, program length, and initial fitness levels, working at 100% VO2Max during HIIT programs increased VO2Max the most compared to other intensities. While there is evidence that there are still benefits seen from HIIT if used at lower intensities (Boyd et al., 2013), the best and most profound benefits are achieved at higher intensities (Acton-Jacobs et al., 2013; Boyd et al., 2013; Buchhat & Laursen, 2013; Cicioni-Kolsky et al., 2013; Moholdt et al., 2013).
Another great feature of HIIT is that it can be utilized by pretty much anyone, and at any fitness level. Both clinical and healthy populations have shown beneficial results from engaging in HIIT programs, aiding individuals with cardiovascular disease, obese and overweight individuals, and even seniors 75+ years old (Boyd et al., 2013, Moholdt et al., 2013). The feasibility of implementing HIIT in these clinical populations, healthy individuals, and high performance athletes, shows how diverse and beneficial this type of exercise can be. So if you’re lacking time to get a ‘full’ workout in, or are tired of running on the treadmill for hours and hours, give HIIT a try, and you should see the same, if not better results from a much shorter workout.
If you want to try a HIIT class out for FREE with me, I run them at Tait Mckenzie, York University. Click here for more details. The group cycling classes I teach also incorporate HIIT throughout and are an excellent high-energy workout. If you want to sign up for these classes or want more information, click here.
References
Acton-Jacobs, R., Fluck, D., Bonne, T.C., Burgi, S., Christensen, P.M., Toigo, M., Lundby, C. (2013). Improvements in exercise performance with high-intensity interval training coincide with an increase in skeletal muscle mitochondrial content and function. Journal of Applied Physiology, doi:10.1152/japplphysiol.00445.2013
Bogdinas, G.C., Stavrinou, P., Fatouros, I.G., Philippou, A., Chatzinikolaou, A., Draganidis, D., Ermidis, G., & Maridaki, M. (2013). Short-term high-intensity interval exercise training attenuates oxidative stress responses and improves antioxidant status in health humans. Food and Chemical Toxicology, doi.org/10.1016/j.fct.2013.05.046.
Buchan, D.S., Ollis, S., Young, J.D., Cooper, S.M., Shield, J.P.H., & Baker, J.S. (2013). High intensity interval running enhances measures of physical fitness but not metabolic measures of cardiovascular disease risk in health adolescents. BMC Public Health, 13, 498-510.
Buchheit, M., & Laursen, P.B. (2013). High-intensity interval training, solutions to the programming puzzle. Part 1: Cardiopulmonary Emphasis. Sports Medicine, 43, 313-338.
Buchheit, M., & Laursen, P.B. (2013). High-intensity interval training, solutions to the programming puzzle. Part 2: Anaerobic energy, neuromuscluar load, and practical applications. Sports Medicine, doi 10.1007/s40279-013-0066-5.
Burgomaster, K.A., et al. (2008). Similar metabolic adaptations during exercise after low volume sprint interval and traditional endurance training in humans. Journal of Physiology, 586 (1), 151-160.
Boyd, C.J., Simpson, C.A., Jung, M.E., & Gurd, B.J. (2013). Reducing the intensity of interval training diminishes cardiovascular adaptation bot not mitochondrial biogenesis in overweight/obese men. PloS ONE, 8(7), e68091. doi:10.1371/journal.pone.0068091
Cicioni-Kolsky, D., Lorenzen, C., Williams, M.D., & Kemp, J.G. (2013). Endurance and sprint benefits of high-intensity and supramaximal interval training. European Journal of Sport Science, 13(3), 304-311.
Daussin, F.N., et al. (2008). Effect of interval versus continuous training on cardiorespiratory and mitochondrial functions: relationship to aerobic performance improvements in sedentary subjects. American Journal of Physiology: Regulatory, Integrative and Comparative Physiology, 295, 264-272.
Faud, O., Schnettker, R., Schulte-Zurhausen, R., Muller, F., & Meyer, T. (2013). High intensity interval training vs. high-volume running training during pre-season conditioning in high-level youth football: A cross-over trial. Journal of Sports Sciences, doi: 10.1080/02640414.2013.792953.
Helgerud, J., et al. (2007). Aerobic high-intensity intervals improve VO2max more than moderate training. Medicine and Science in Sports and Exercise, 39(4), 665-671.
Horowitz, J.F., & Klein, S. (2000). Lipid metabolism during endurance exercise. American Journal of Clinical Nutrition, 72, 558-563.
LaForgia, J., Withers, R.T., & Gore, C.J. (2006). Effects of exercise intensity and duration on the excess post-exercise oxygen consumption. Journal of Sports Science, 24(12), 1247-1264.
MacDougall, J.D., et al. (1998). Muscle performance and enzymatic adaptations to sprint interval training. Journal of Applied Physiology, 84(6), 2138-2142.
Moholdt, T., Madssen, E., Rognmo, O., & Aamot, I.L. (2013). The higher the better? Interval training intensity in coronary heart disease. Journal of Science and Medicine in Sport, doi.org/10.1016/j.jsams.2013.07.007
Perry, C.G., et al. (2008). High-intensity aerobic interval training increases fat and carbohydrate metabolic capacities in human skeletal muscle. Applied Physiology, Nutrition, and Metabolism, 33(6), 1112-1123.
Talanian, J.L., et al. (2007). Two weeks of high-intensity aerobic interval training increases the capacity for fat oxidation during exercise in women. Journal of Applied Physiology, 102(4), 1439-1447.
Tjonna, A.E., Leinan, I.M., Bartnes, A.T., Jennsen, B.M., Bibala, M.J., Winett, R.A., & Wisloff, U. (2013). Low- and high-volume of intensive endurance training significantly improves maximal oxygen uptake after 10-weeks of training in healthy men. PloS ONE, 8(5): e65382. doi:10.1371/journal.pone.0065382.
Slørdahl, S.A., et al. (2004). Atrioventricular plane displacement in untrained and trained females. Medicine & Science in Sports & Exercise, 36(11), 1871-1875.
Sloth, M., Sloth, D., Overgaard, K., & Dalgas, U. (2013). Effects of sprint interval training on VO2max and aerobic exercise performance: A systematic review and meta-analysis. Scandinavian Journal of Medicine & Science in Sports, doi: 10.1111/sms.12092.
Zuhl, M. & Kravitz, L. (2012). HITT vs. continuous endurance training: Battle of the aerobic titans, IDEA Fitness Journal, 9(2).